High moderate and low. Z Only one physicianNPP may bill for CCM.
Creating A Chronic Care Management Patient Brochure 7 Topics To Cover
Physicians Clinical Nurse Specialists Nurse Practitioners and Physician Assistants may bill for this service.
. CCM services are only available to patients with two or more chronic conditions. Benefits of CCM Services. In designing its CCM TeamHealth focused on three quantitative analytics to track over time.
We believe that patient and family involvement and access to records are critical elements in achieving positive outcomes. LET US KNOW HOW TO REACH YOU OR CALL US AT 800-376-0212 CONTACT US CCM Offering Brochure Learn How CareVitalitys Turnkey Chronic Care Management CCM Offering contributes to better health and care for individuals reduced spending improved reimbursement and improved cost and quality scores under the Quality Payment Program. I am able to work with you as you identify your own health goals and areas that you would like to focus on to manage your insert chronic disease diagnosis.
Next TeamHealth looks at fall risk breaking them into three categories. Give your care manager information to help support your care. Approximately 4291 per Patient per Month.
Encourage them to talk to a representative from your organization who can give them a more personalized breakdown of estimated costs. Patient Responsibilities You are responsible to. Medicare defines a chronic condition as a condition that is expected to last for at least 12 months and that increases the risk of death acute exacerbation of disease or a decline in function.
CHRONIC CARE MANAGEMENT CCM z CPT 99490 is billed when at least 20 minutes of clinical staff time is spent in care management activities in a calendar month. Greater energy less pain and reduced fatigue. Incline Village Community Hospital.
Selling Chronic Care to Patients 1. This consists of a series of either phone calls or visits with me 2. Agree to work with a care manager.
45month z Patients must have w 2 or more chronic conditions. It may be best to draft a basic letter that the physician can review with the patient during their face-to-face visit prior to billing for the CCM. Chronic care management CCM is a Medicare Part B benefit for patients with two or more chronic conditions delivered under the supervision of a physician or non-physician provider ie nurse practitioner or physician assistant.
Chronic care management is beneficial for patients in terms of ongoing health and wellness support increased access to appropriate medical resources enhanced communication with members of their care team reduction in emergency room visits and hospitalization or readmissions and increased engagement in their own healthcare. Do your best to follow your care plan. Each patients use of antipsychotics which TeamHealth logs and analyzes.
Chronic care management services may include. According to the Department of Health and Human Services chronic care management is the provision of care management and coordination services to patients with two or more chronic conditions Examples of chronic conditions include but are not limited to. CCM Documentation Requirements In order to bill for CCM you must provide the following documentation.
I provide support for patients that have a chronic disease diagnosis. Alzheimers disease and related dementia Arthritis osteoarthritis and rheumatoid Asthma. Chronic care management CCM is defined as.
Chronic care management services to you. 1 Medicare requires that the patient understands and agrees to the chronic care management services before they are offered and billed. Having a customized action plan designed to improve your health.
At least 20 minutes a month of CCM services Personalized assistance from a dedicated health care professional who will work with you to create a care plan Coordination of care between your pharmacy specialists testing centers hospitals and more 247 emergency access to a health care professional. Health System Mailing Address. Proven benefi ts of chronic care management Several studies document the proven benefi ts of participating in a chronic care management program including.
Chronic conditions put the patient at significant risk and they need more management than the practice can provide in the clinic. 20-60 minutes of care coordination per month Completed remotely in addition to regular office visits Guided by the development of a care plan Medicare considers patients eligible for chronic care management if they have multiple two or more chronic conditions expected to last at least 12 months. Z Covers a calendar month.
Cost of chronic care management In the brochure its wise to explain to patients that CCM is covered by Medicare and typically incurs minimal out-of-pocket cost. Let your care team know if you cannot follow your plan. Ask questions when you hear or read something you do not understand.
Who Can Bill For It. View full list of our locations. CCM services are extensive including structured recording of patient health information an electronic care plan addressing all health issues access to care management services managing care transitions and coordinating and sharing patient information with practitioners and providers outside the practice.
The goal of the program is to help you manage your health with the help health experts in between your doctor visits. Or other qualified health care professional per calendar month with the following required elements. NEW PROGRAM designed to help KEEP YOU OUT OF HOSPITAL 2.
Chronic care management provides health benefits to patients and financial benefits to providers but in order to get paid its important for your team to perform chronic care management documentation according to CMS guidelines for the program. Provides 24 HOUR ACCESS to your health care team. What does it Pay.
Tahoe Forest Health System. Multiple two or more chronic conditions expected to last at least 12 months or until the death of the patient chronic conditions place the patient at significant risk of death acute exacerbation decompensation or functional decline. 4 Patient Benefits Patients and their caregivers will gain a team of dedicated health care professionals who can help them plan for better health and stay on track - Services such as monthly check-ins and ready access to their care team improves their care coordination including improved communication and management of care transitions.
Fewer social role limitations. 1 day ago3 datapoints every post-acute provider should study. Allows time to take BETTER CARE of you.
We have developed a robust program that allows our diverse team of health care professionals administrators and support staff to ensure our chronic care management delivery exceeds the current standards of care.

Chronic Care Management Patients Nebraska Health Network

Chronic Care Management Path To Patient Centered Care Coordination

Winter 2017 January March By Missouri Academy Of Family Physicians Issuu

Chronic Care Management Ccm Catalina Island Medical Center
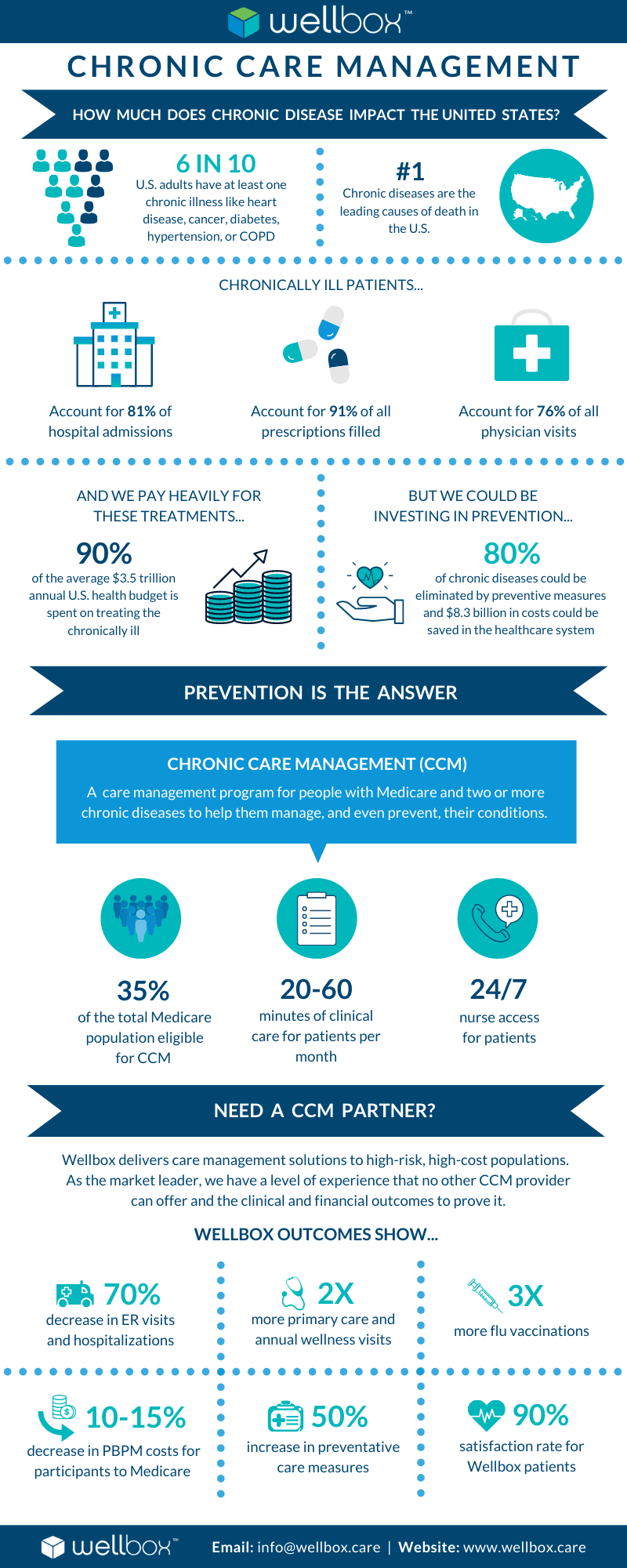
16 Facts You Should Know About Chronic Care Management Wellbox
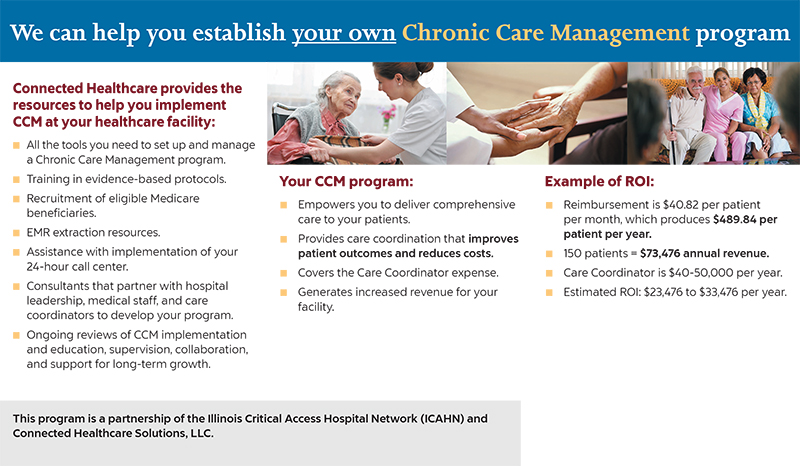
Chronic Care Management Program Connected Healthcare Solutions
Chronic Care Management Documentation Best Practices
Chronic Care Management Nebraska Health Network
0 comments
Post a Comment